Dr. Ebraheim’s educational animated video describing fractures of the ankle and the surgical treatment.
Educational video describing fractures of the ankle X - rays.
It describes ankle fracture classification, ankle fracture dislocation.
It also describes ankle fracture treatment and ankle fracture surgery and ankle fracture recovery
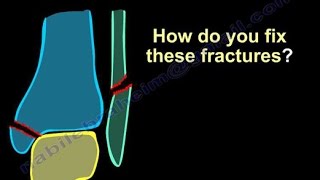
You start fixing these fractures by fixing the fibula, the fibula is the key for the ankle stability, when you fix it you need to provide length and stability to the ankle joint, except in 2 situations:
1- Supination adduction injury: you will do the medial side first because the fibula is short and fixation of this will not give you enough stability, you need to go after the joint injury first, which is the fracture of the medial malleolus, and you fix that by antiglide plate (buttress plate) or by screws parallel to the joint.
2- When the fibular fracture is comminuted, so that will facilitate positioning of the talus within the mortise and will help to achieve anatomic reduction of the fibula, the line of the articular surface of the talus should be parallel to the ankle (shenton’s line), the dime sign is interrupted.
How do you fix the fibula?
By regular lateral plate, but that can cause irritation of the soft tissue, there may be violation of the joint as the screws may be so long.
I like to get the mortise view to be able to see the screws, contrary to the medial malleolar screws; I like to get an AP view to see if these screws are violating the joint.
Usually this plate is a neutralization plate after you do lag screw for the fracture itself.
The second method is the antiglide technique and that’s the buttress plate posteriorly, so it is a posterior technique that means if you go distal you may irritate the peroneal tendons or you may injure the posterior peroneal retinaculum, this technique is biomechanically superior to the regular plate technique.
• In the pronation – external rotation: you will do probably lag screws followed by neutralization plate.
• In the pronation abduction injury: you probably will do the classic operation, try to test the syndesmosis, because it is very important, and if the fibular fracture is comminuted, then I will start by exposing, reducing and fixing the medial side first.
• Supination – external rotation: do reduction then lag screws and neutralization plate fixation, this plate can be applied lateral or posteriorly.
When to do the surgery? What is the timing of the surgery?
Usually when the ski condition permits, when the skin wrinkles are present and the abrasions becomes epithelialized and no bacteria on skin surface.
The wrinkle sign will be present when all the interstitial edema has left the skin and tissues.
It may take 2-3 weeks to get the wrinkle sign.
Become a friend on facebook:
[ Ссылка ]
Follow me on twitter:
[ Ссылка ]
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
[ Ссылка ]