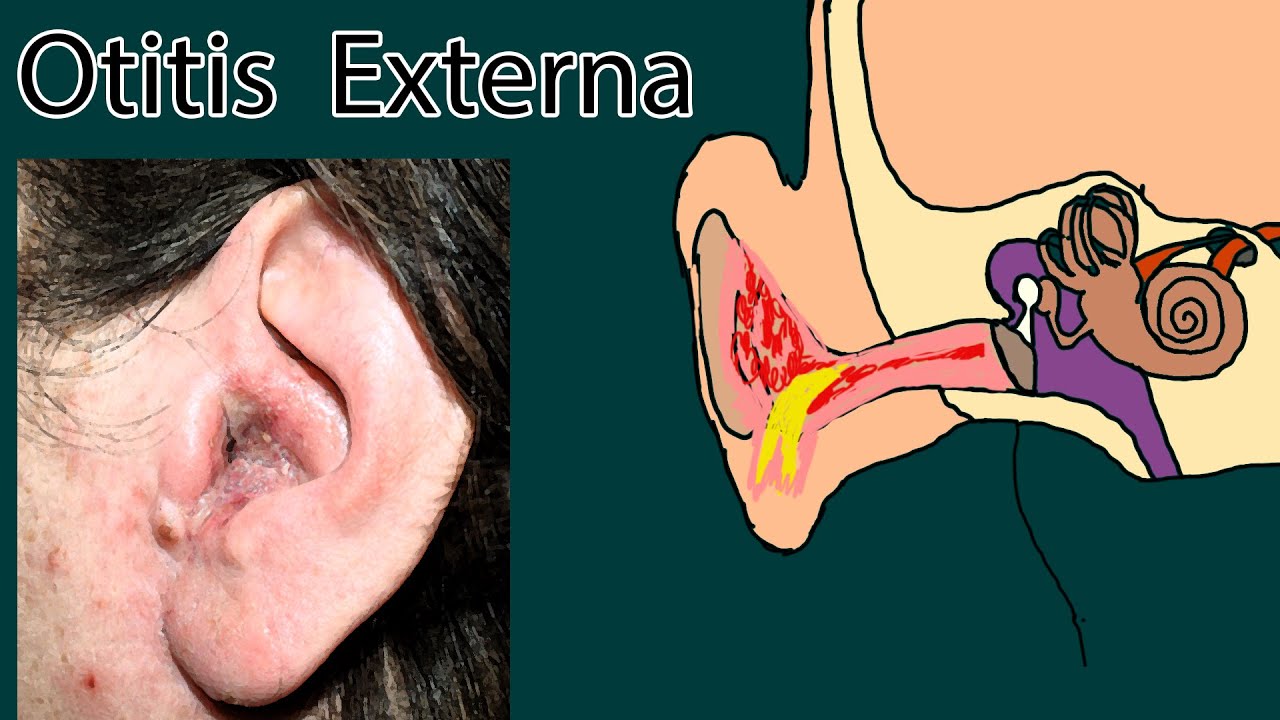
External otitis also called as swimmer’s ear.
It is pain and inflammation outer part of the ear.
Other symptoms include:
Ear pain, swelling of the ear canal, and occasionally decreased hearing.
Pain can be constant, or occur during ear movement. Hight temperature is not common for external otitis.
Itching called pruritis commonly presented. Also common purulent discharge.
Patient frequently has recent history of recent water exposure. Or phisicaltrauma.
Most external otitis is caused by bacterias, usually gram negative rods. Such as pseudomonas and proteus.
Sometimes it is caused by fungi, for example aspergillus, which grows in presence of excessive moisture.
If the patient is immunocompromised or with uncontrolled diabetes, it can have inflammation not only outer ear, but also skull base, inflammation of bones, called osteomyelitis.
Manipulation of the ear causes pain.
Ear canal can be erythematous and very edematous, sometimes not possible to visualize tympanic membrane.
The treatment of external otitis involves protection of the ear from additional moisture and avoid further mechanical injury.
Acidification with a drying agent. For example 50/50 mixture of isopropyl alcohol/white vinegar.
When infected antibiotic solution or suspention:
Aminoglycoside: Neomycin/polymyxin B.
Fluoroquinolone, for example ciprofloxacin.
Purulent debris filling the ear canal should be gently removed to permit entry of the topical medication.
Drops should be used abundantly. 5 or more drops 3 or 4 times a day.
In Severe cases oral Fluoroquinolone, for example ciprofloxacin 500 mg twice daily for 1 week, should be used .
Fluoroquinolones are effective against pseudomonas.
Treatment of “malignant external otitis” requires prolonged antipseudomonal antibiotic administration, often for several months.
Swimmer's Ear (Otitis Externa): Causes, Diagnosis, Treatment
Теги
earear painexternal ear painauter ear painouter ear painear inflamationotitis externa dog treatment homeotitis media and otitis externamalignant otitis externacan otitis externa turn into otitis mediaotitis externa ear drops not workingotitis externa symptoms jaw painotitis externa ear drops bnfotitis externa ear drops ukotitiotitis externaotitis externa treatmentotitis treatmentear dropsear pain after swimmingswimmers ear





































































![Протоколы Сионских Мудрецов - Библия Гитлера [БЕСТИАРИЙ]](https://i.ytimg.com/vi/QEPXqtuHrLM/mqdefault.jpg)



