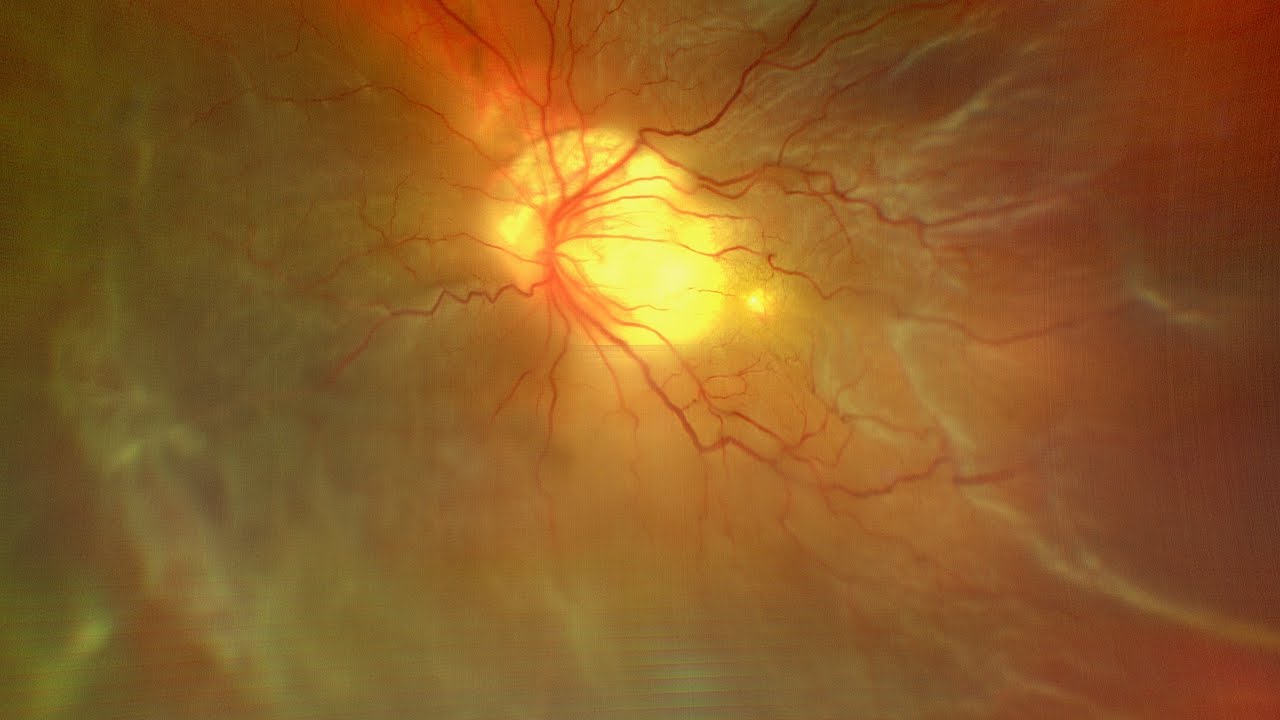
Macular hole in combination with retinal detachment typically occurs in one of two scenarios. The first of these is in the presence of high myopia and staphyloma. In these cases, the macular hole is the break that led to the retinal detachment. This detachment is typically posterior but can spread anteriorly, and generally there are no other associated breaks.
There is a rhegmatogenous retinal detachment, which started with a peripheral break or breaks and subsequently spread posteriorly. The stretching of the retinal tissue over the thin fovea during detachment has led to the formation of the macular hole.
Both scenarios require the macular hole to be fixed. The surgical approach for macular hole in combination with retinal detachment is slightly different from and more challenging than surgery for a typical macular hole without concurrent retinal detachment. The primary challenge is peeling the internal limiting membrane (ILM) over the detached and mobile retina. Further, there is the additional potential risk of dye gaining access to the subretinal space under the detached retina and causing toxicity.
Challenges associated with surgery in high myopia include long axial length, staphyloma and, in some eyes, decreased contrast due to light pigmentation.
Retina today January/February 2018